
Biotechs like Cellectis, Juno Therapeutics and Kite Pharma have all faced patient deaths in clinical trials for their CAR-T cell immunotherapies for cancer. In an effort to address these side effects, clinicians at The University of Texas MD Anderson Cancer Center have published new guidelines in the journal, Nature Reviews Clinical Oncology, which could help in the management of these toxicities.
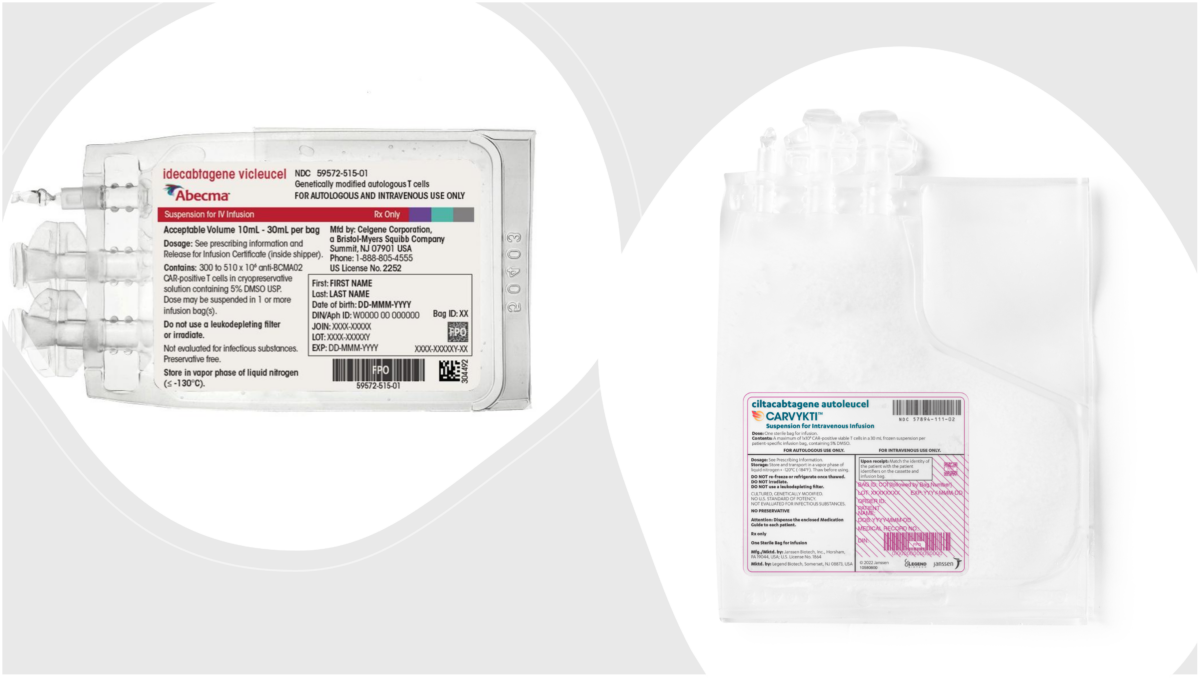
CAR-T cell immunotherapy uses engineered patient-derived immune cells to help the body’s natural defense mechanisms recognize and destroy cancer cells. While the therapeutic approach has shown particular promise in treating blood-based cancers, the recent string of patient deaths has called the drugs’ safety into question.
“CAR-T cells provide an entirely new level of improved disease response among patients with certain blood cancers and hold promise for more wide-ranging use,” said Dr. Elizabeth Shpall, deputy chair and professor of Stem Cell Transplantation and Cellular Therapy at MD Anderson. “The algorithms that we published are conservative, detailed, and will help us save lives as we move forward with these exciting but also more toxic therapies.”
In addition to research conducted by other institutions, the review paper includes data from over 100 patients treated with CAR-T therapies currently being developed to treat leukemia and lymphoma. These therapies – which target the CD19 protein present on certain cancer cells – have shown treatment response rates between 50 and 90 percent in patients who have previously been unresponsive to traditional cancer therapies.
“There have been no new treatments approved for patients with aggressive B-cell lymphomas relapsing after first line therapy in 30 years, and only about 10 percent survive long term,” said Dr. Sattva Neelapu, professor of Lymphoma and Multiple Myeloma. “Existing second-line treatments, combination chemotherapy followed by autologous stem cell transplant when possible, take three to six months – CAR T cell therapies take a few weeks.”
The review focused on prevention and treatment of two side effects of CAR-T immunotherapy: cytokine release syndrome (CRS) and CAR-T-cell-related encephalopathy syndrome (CRES). Both conditions can be fatal, highlighting the need for faster response to early symptoms of the adverse events.
The researchers provided recommendations on patient pre-treatment with chemotherapeutic agents, as well as guidelines as to how patients should be monitored during, and directly following, infusion with the CAR-T cells. Should patients begin to exhibit early symptoms of CRS or CRES, the researchers present information on how their condition can be assessed and what treatments should be administered based on the severity of the adverse event.
“We need longer term follow up of patients treated so far in clinical trials, but these are potentially curative treatments,” Neelapu said. “The toxicities are unique, and every member of the care team needs to be trained to recognize them and act accordingly.”






Join or login to leave a comment
JOIN LOGIN