Idiopathic pulmonary fibrosis (IPF) remains one of the most challenging diseases in respiratory medicine.
Characterized by progressive scarring of lung tissue and an irreversible decline in lung function, IPF carries a prognosis worse than many common cancers. Yet despite its severity, the disease has long flown under the radar, often diagnosed late, misidentified as other respiratory or cardiac conditions and treated with limited therapeutic options.

and Head of the Therapeutic Area Inflammation
Boehringer Ingelheim
In this Xtalks Clinical Edge interview, Martin Beck, Corporate Senior Vice President and Head of the Therapeutic Area Inflammation at Boehringer Ingelheim, discussed how the field’s understanding of IPF is shifting, and why earlier diagnosis, better disease characterization and more patient-centric clinical research are critical to improving outcomes.
Delayed Diagnosis: A Persistent and Costly Gap
One of the most pressing unmet needs in IPF care remains early and accurate diagnosis. Initial symptoms, such as chronic cough, fatigue and shortness of breath during routine activities, are often subtle and easily attributed to aging, asthma, chronic obstructive pulmonary disease (COPD) or cardiovascular disease.
“Awareness of pulmonary fibrosis is underserved,” Beck explained. Many patients are diagnosed too late, when significant lung function has already been lost.
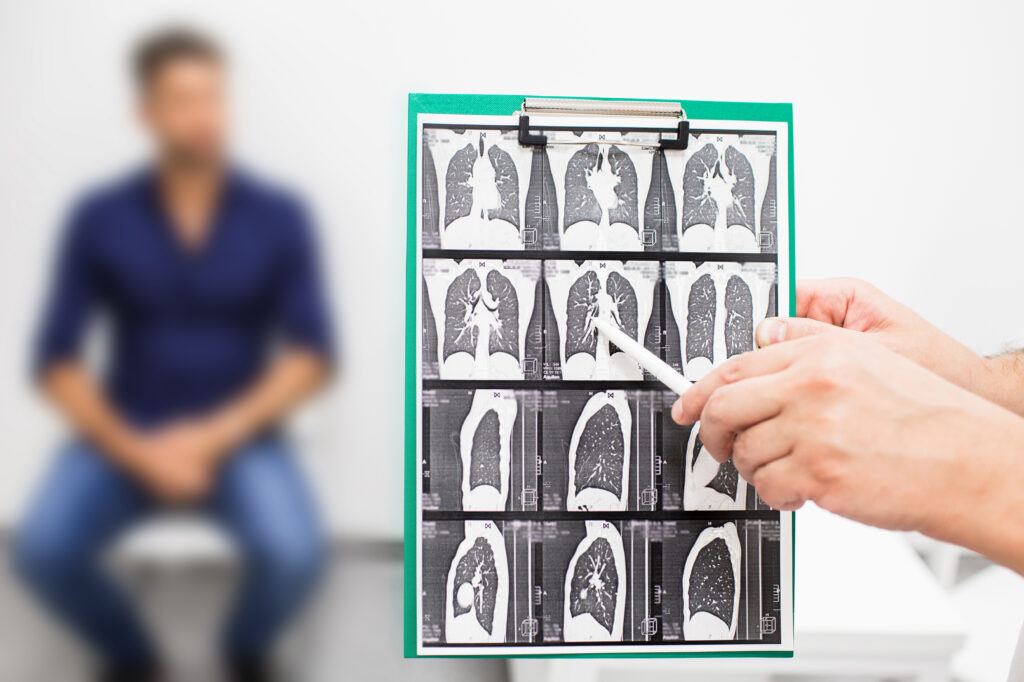
High-resolution computed tomography (HRCT) scans remain the gold standard for diagnosis, but even then, early fibrotic changes can be difficult to detect. Missed or delayed referrals to specialist centers further compound the problem. This delay is particularly detrimental in a disease where lung damage cannot be reversed.
As a result, there is growing interest in technologies that can identify disease earlier and more reliably. Artificial intelligence (AI)-driven imaging tools are emerging as a promising solution, enabling radiologists to detect subtle, early scarring patterns that might otherwise go unnoticed. These approaches could ultimately shift IPF diagnosis upstream, allowing treatment to begin sooner and potentially slowing disease progression earlier in the course.
A Heterogeneous and Systemic Disease
Once thought of primarily as a localized fibrotic lung disorder, IPF is increasingly recognized as a heterogeneous disease with systemic features. This complexity has significant implications for both therapeutic development and clinical trial design.
IPF exists alongside related conditions under the broader umbrella of progressive pulmonary fibrosis (PPF), where fibrosis develops secondary to underlying diseases such as rheumatoid arthritis, scleroderma or sarcoidosis.
While antifibrotic therapies have formed the backbone of treatment, growing evidence suggests that inflammation, immune dysregulation and vascular processes also play meaningful roles, particularly in non-idiopathic forms of progressive fibrosis.
“Our understanding of the biology and the background of the disease has advanced over time,” Beck said. There is now recognition that it isn’t just a single-pathway disease. There are inflammatory, fibrotic and even vascular components that may all contribute to the pathology of the disease.
This evolving biological insight has driven a more nuanced approach to drug development, emphasizing mechanisms that can address multiple aspects of disease pathology rather than fibrosis alone.
Beck explained that the focus now is on truly understanding the disease and finding opportunities to tackle the disease in a more holistic manner.
Read Xtalks Clinical Edge™ Issue 7
Xtalks Clinical Edge is a magazine for clinical research professionals and all who want to be informed about the latest trends and happenings in clinical trials. This magazine immerses you in a world where industry leaders, patient advocates and top researchers converge to provide the most insightful perspectives on clinical trials.

Implications for Clinical Trial Design
The recognition of IPF as a heterogeneous condition has also reshaped how clinical trials are structured. Over the past decade, trial designs have expanded from narrowly defined IPF populations to include broader fibrosing interstitial lung diseases, with regulatory agencies increasingly acknowledging these distinctions.
Patient selection, disease stratification and endpoint selection are now more tightly aligned with underlying disease biology. However, designing trials in this space remains challenging, particularly given the burden placed on patients who are often older, symptomatic and living with a life-limiting illness.
To address this, developers are incorporating patient input directly into trial design. Beck highlighted the growing role of patient advocacy groups in co-creating trial materials, refining consent forms and simulating trial participation to identify unnecessary complexity.
“From a scientific and regulatory perspective, a trial may look perfect,” he noted. “But for patients, it can be overwhelming, impractical or very difficult.” Patient feedback can help bridge these gaps.
Digital tools are also beginning to ease trial participation. Wearables that objectively track symptoms such as cough, for example, reduce reliance on patient self-reporting while generating more precise data. Simplified communication tools, including video-based consent and clearer trial explanations, are helping reduce friction without compromising scientific rigor.
“The more objective we can be by applying innovation in clinical trials, the better it helps us to truly understand the effect that we have on patients’ lives,” Beck said.
Moving Beyond Traditional Endpoints
Forced vital capacity (FVC) has long served as the primary surrogate endpoint in IPF trials, reflecting lung function decline over time. While useful, FVC alone does not fully capture the lived experience of patients or the ultimate goal of therapy: extending survival and preserving quality of life.
There’s growing recognition that we need to look beyond surrogates, Beck explained. “Mortality and survival benefits, as well as exacerbation and hospitalization, are critically important clinical outcomes. FVC is only a surrogate parameter like blood pressure or blood sugar.”
Advanced imaging analytics may also play a larger role in the future, offering a window into microscopic disease progression before measurable functional decline occurs.
Patient-reported outcomes, while valuable, present challenges due to variability. Additionally, in a disease where stabilization and improvement would be the desired outcomes, benefits such as the slowing of disease progression can be harder for patients to perceive.
Towards Innovation-Driven Change
Despite these challenges, the IPF field is entering a period of renewed momentum. Advances in disease biology, imaging, digital health and therapeutic development are converging to create new opportunities for patients who have long faced limited options.
Perhaps most encouraging is the shift toward earlier intervention and individualized disease monitoring, enabled by better diagnostic tools and a deeper understanding of disease trajectories. Combined with a stronger emphasis on tolerability and long-term treatment adherence, these advances may finally begin to bend the curve in a disease where progress has historically been slow.
“Earlier diagnosis, earlier treatment and better patient characterization using technologies that improve diagnosis and monitor disease progression earlier on is where the field is heading,” Beck said. “And that’s where we have the greatest opportunity to make sure patients get the best treatment possible.”








Join or login to leave a comment
JOIN LOGIN