
Over the last decade, immuno-oncology agents have been stealing the cancer therapeutic spotlight. About 940 clinical stage agents have been identified for more than 270 different targets, and at least 12 new immuno-oncology agents have been approved by the US Food and Drug Administration (FDA). Today, immuno-oncology agents are considered standard of care for at least 15 different cancer types.
A wide variety of immuno-oncology agents have burgeoned from a greater understanding of the immune response and cancer pathology. Some agents lead to non-specific activation of the immune system (immune checkpoint inhibitors), while others enhance responses to specific cancer antigens (adoptive cellular therapies). Newer agents like oncolytic viruses and cancer vaccines boast even greater specificity and potency.
As more agents approach the clinic, it is imperative for researchers to consider the design and conduct of immuno-oncology clinical trials. Given the diversity of agents in this newly tapped field, researchers may encounter unique challenges for site selection, patient selection, biomarker selection and imaging for assessing patient responses.
To learn more about challenges and considerations in designing and conducting immuno-oncology clinical trials, watch this on-demand webinar from Medpace, a global clinical contract research organization.
Site Selection
Experience with immuno-oncology agents is a key factor in site selection. Consider the development of chimeric antigen receptor (CAR) T therapy. Typically, this involves collecting cells from patients, engineering CAR T products at a lab and re-infusing them back into the patient at a treatment site. Coordinating schedules, tracking sites, overseeing product storage (ex. cryopreservation) and monitoring patients every step of the way requires highly trained personnel and clearly defined processes.
For cellular therapies, in particular, researchers should also consider selecting sites that are accredited by agencies that set standards for performing cell transplantation and therapy. In Canada, Australia and the US, sites can receive accreditation from the Foundation for the Accreditation of Cellular Therapy (FACT).
“If sites are accredited, it provides a layer of external validation that the sites are likely to meet all the appropriate quality mechanisms for conducting a transplant or cellular therapy trial,” said Dr. Gregory Hale, Senior Medical Director of Hematology & Oncology at Medpace. “If sites are not accredited, then the onus is on the investigator to ascertain whether or not the site is appropriate.”
Finally, site personnel should also be educated on and trained to address adverse events or toxicities. Unlike chemotherapy, most adverse events and toxicities related to immuno-oncology agents are not dose-related and could potentially occur long after the therapy is administered.
Most non-targeted therapies like immune checkpoint inhibitors can result in generalized inflammation and autoimmunity, which can be managed with corticosteroids if identified early. However, sites need to define a standardized system for grading and treating toxicities. For example, site personnel need a systematic way to rule out hepatitis caused by viral infection rather than by the immuno-oncology agent itself. The team must also know when to discontinue immuno-oncology therapy and initiate treatment for toxicities.
Immune checkpoint inhibitors are also associated with neurologic, endocrine and renal toxicities which require the attention of specialists. Dr. Hale emphasizes that sites should have a clearly defined mechanism for involving specialists and physicians who are not directly involved in the oncology team.
Patient Selection
In almost all clinical trials, researchers must consider patient age, weight, sex, co-morbidities and other lifestyle factors that could affect a treatment’s efficacy. For some cancer trials, only patients with a certain cancer type and/or genetic mutation may be eligible. In immuno-oncology trials, researchers must consider at least three more variables in defining patient eligibility criteria.
Prior immunotherapy treatment
“With more approved products, it’s harder to find patients who are not naïve to these types of products,” said Dr. Hale.
Prior exposure to immunotherapies may potentially enhance or mitigate the effects of the treatment being tested. Additionally, immuno-oncology treatment may exacerbate symptoms of people with autoimmune diseases.
Refractoriness to standard therapy
Trials evaluating immuno-oncology agents might seek out patients who are refractory to first-line treatment or single-agent immunotherapy. Individuals who do not respond to single-agent immunotherapy might be eligible for trials evaluating a combination therapy.
Pediatric Populations
Testing immuno-oncology agents in pediatric populations pose additional regulatory and ethical considerations. In studying pediatric populations, researchers must establish validated clinical endpoints, biomarkers and scoring systems that may differ from adult populations.
Biomarker Selection
Compared to chemotherapy or targeted therapy, immuno-oncology biomarker selection strategies can be far more complex. Ideally, the chosen biomarkers should monitor components of the immune system and tumor microenvironment but also measure additional factors that could affect both.
One of the most well-known biomarkers in immuno-oncology is PD-L1, an immune regulatory protein. The interaction between PD-L1 and its receptor PD-1 (found on activated T cells) functions to maintain homeostasis by modulating the immune response. However, this same interaction shuts down anti-tumor activity when PD-L1 on cancer cells engage with PD-1 on T cells. Upregulation of PD-L1 in cancer cells is widely believed to help cancers evade the immune system.
While nearly all human tumors express PD-L1 to some degree, cancers associated with higher levels of PD-L1 may be more susceptible to immune checkpoint inhibitor therapy. Keytruda (pembrolizumab), one of the earliest immune checkpoint inhibitors to enter the market, was first indicated for patients with non-small cell lung cancer — a disease in which 45-50 percent of cancer cells express PD-L1. Keytruda is also indicated for melanoma, which typically expresses PD-L1 in 40 percent of its cells.
Given the ubiquity of this immuno-oncology biomarker, many pharmaceutical companies have developed their own assays and treatments targeting PD-L1/PD-1. But, according to Dr. El Mustapha Bahassi, Associate Director of Clinical Laboratory at Medpace, this may pose a significant problem.
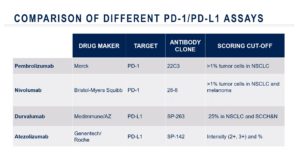
“The problem is, each one of these companies has established different scoring cut-offs to define what is positive expression,” said Dr. Bahassi. “All this led to multiple challenges related to mapping of assays and cut-off values and therapies that are complicated and highly dynamic.”
There is a need for assay standardization and automated solutions, he added. Additionally, PD-L1 expression is not always correlated with response to immune checkpoint inhibitor therapy. Some low-expressing PD-L1 cancers are highly responsive to immune checkpoint inhibitors while some highly expressing PD-L1 cancers are less responsive.
In addition to PD-L1, researchers should also examine biomarkers indicative of pre-existing immunity.
According to Dr. Bahassi, “Patients whose tumors are already infiltrated by killer T cells typically experience better outcomes and are more likely to respond to PD-L1 checkpoint immunotherapy.”
Tumor mutational burden and the gut microbiome may also predict a patient’s response to immune checkpoint inhibitors. For the former, a higher number of somatic mutations means more targets for the immune system: skin, blood and lung cancers have a high tumor mutational burden and are typically responsive to immune checkpoint inhibitors. For the latter, a highly diverse gut microbiome is predictive of patient response to immune checkpoint inhibitors.
While no single biomarker is perfect, each provides important predictive, pharmacodynamic and prognostic information.
“There is a need for a more integrated approach to biomarkers in immuno-oncology,” said Dr. Bahassi. “All this will require advanced bioinformatics tools, machine learning and artificial intelligence … this is a work in progress.”
Assessing Patient Response Through Imaging
Imaging is a common way to assess patient response to therapy in an oncology trial. For common imaging modalities like CT scans and MRI, oncologists can refer to Response Evaluation Criteria in Solid Tumors (RECIST) to track patient response. Responses can be classified as complete response, partial response, stable disease or progressive disease based on changes to lesion measurements relative to baseline.
In 2009, the new and simplified RECIST 1.1 was introduced. This new version limited the number of target lesions to be measured and incorporated FDG/PET imaging for detecting glucose metabolism in cancer cells.
Both RECIST 1.0 and RECIST 1.1 are useful for classifying patient responses to traditional chemotherapeutics but are not appropriate for assessing responses to immuno-oncology agents.
“Radiographic responses in immuno-oncology are unlike responses to chemotherapy where tumor cell killing and shrinkage are more immediate,” said Dr. Jess Guarnaschelli, Medical Director of Hematology & Oncology at Medpace.
Immuno-oncology agents may result in a flare effect, thought to be due to an infiltration of T cells into the tumor. This infiltration may increase the size of the tumor at first before diminishing at a later time point, giving the impression of a “pseudoprogression” of the malignancy.
irRC, PERCIST, irRECIST, iRANO and iRECIST are some guidelines that account for the immune response patterns seen with immunotherapies.
In iRECIST, the bar is “reset” if RECIST progressive disease is followed by tumor shrinkage at the next time point measurement. Therefore, RECIST 1.1-classified progressive disease is called immune unconfirmed progression of disease according to iRECIST. At subsequent time points, target lesions can be classified as immune stable disease, immune partial response and immune confirmed progressive disease.
Currently, RECIST 1.1 is used as the primary criteria for response-based endpoints in randomized studies planned for licensing applications while iRECIST is considered exploratory. Without the appropriate imaging endpoints, oncology trials may fail or be terminated early.
In designing and conducting immuno-oncology clinical trials, it is important to keep in mind the unique challenges presented with these forms of therapy. Ultimately, these considerations can help improve clinical trial success and bring more novel treatments to patients who need them.
Dr. Gregory Hale, Dr. El Mustapha Bahassi and Dr. Jess Guarnaschelli share more insights on immuno-oncology clinical trials in this on-demand webinar.
This article was created in collaboration with the sponsoring company and the Xtalks editorial team.






Join or login to leave a comment
JOIN LOGIN