Finding biomarkers for solid tumors used to be limited to tissue samples collected with a tissue biopsy.
Now, biomarkers obtained from liquid biopsy samples like blood, cerebrospinal fluid or urine may help with cancer treatment selection and monitoring of treatment outcomes.
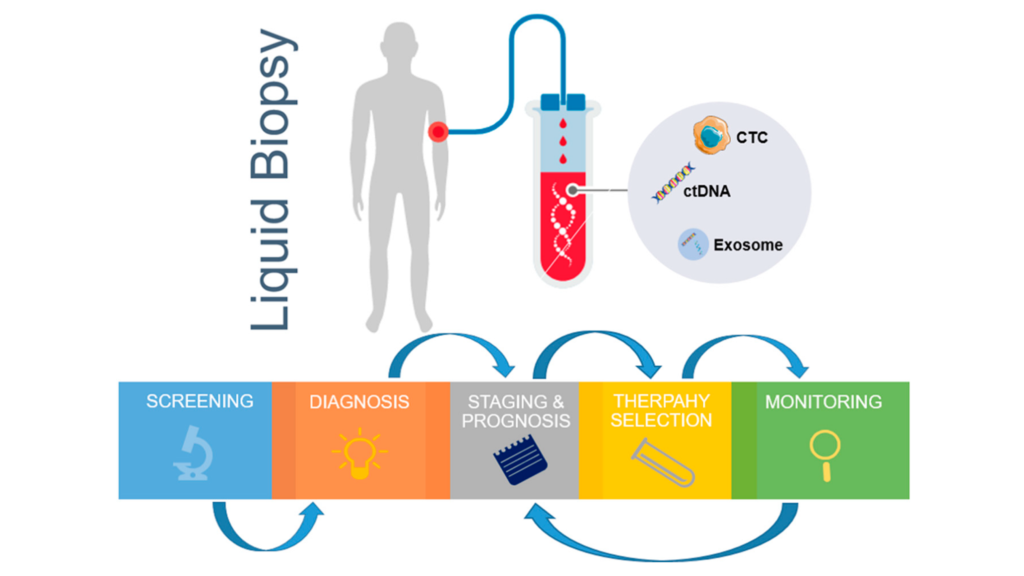
Liquid biopsy tests in oncology involve isolating entities such as circulating tumor cells (CTC), circulating tumor DNA (ctDNA) and tumor-derived exosomes. These tumor-derived entities are used to derive genomic and proteomic data.
Such information can reveal details about tumor staging, tumor progression, heterogeneity, gene mutations and clonal evolution.
In addition, liquid biopsy is a minimally invasive technology and has a much lower risk compared to tissue biopsy procedures.
“Liquid biopsies have demonstrated promising activity in multiple clinical settings, but the great enthusiasm and expectations around them can be harmful if not adequately managed,” said Dr. El Mustapha Bahassi, PhD, Director, Clinical Laboratory Sciences, at the global clinical research organization (CRO) Medpace.
In a recent webinar, Dr. Bahassi reviewed the current methodologies involved in liquid biopsies and the utility of three liquid biopsy biomarkers — CTCs, ctDNA and exosomes — in cancer management and predicting outcomes. The same webinar held a Q&A session with Dr. Bahassi and two other experts from Medpace, Dr. Lyon L. Gleich, MD, FACS, Senior Vice President, Medical Department, and Dr. Christopher Huth, PhD, Senior Clinical Trial Manager, Clinical Trial Management.
Watch the free, on-demand webinar to gain insights from a group of experts about the current opportunities and challenges of liquid biopsy in oncology.
Liquid Biopsy Use in Oncology Clinical Trials
According to Dr. Bahassi, a recent survey on the ClinicalTrials.gov database in September 2022 showed that of the ongoing clinical trials using liquid biopsy in oncology, there are 2,988 studies involving CTCs, 1,025 studies using ctDNA, 608 studies using cell-free DNA (cfDNA) and 15 studies using exosomes.
“Recent clinical trials using liquid biopsy have shown encouraging results for the early detection of cancer and established that liquid biopsy biomarkers are a good technique for the surveillance of disease progression, real-time monitoring of possible therapy resistance and improvement of treatment,” said Dr. Bahassi. “This will translate into a better quality of life and extended progression-free survival and overall survival for cancer patients.”
CTC-Based Liquid Biopsy in Oncology
Circulating tumor cells (CTCs) are tumor cells that shed from sites of primary and metastatic cancer and travel through the bloodstream.
CTCs are more abundant in late-stage cancer and less abundant in early-stage cancer.
Concentration of CTCs in Cancer Patients
There are between 0 to 10 CTCs per mL of blood in early-stage cancers versus thousands of CTCs per mL of blood in conditions like metastatic carcinoma. The concentration of CTCs in blood can vary depending on cancer type. For example, gliomas shed very little CTCs in circulation compared to colorectal cancer.
According to Dr. Bahassi, the method of CTC isolation can make a big difference in terms of the number of CTCs that are enumerated. For instance, there is a difference in CTC separation based on epithelial surface markers compared to CTC separation based on size and morphology.
CTC Isolation Techniques
There are several methods currently used to isolate CTCs, but Dr. Bahassi emphasized that each one of those methods has its own challenges that limit its clinical implementation.
Immunofluorescent staining of CTCs is a CTC isolation method that has been used since the first US Food and Drug Administration (FDA) approval in 2013 for the CellSearch® CTC enumeration platform. Immunofluorescent staining of CTCs uses epithelial or tumor cell surface markers such as epithelial cell adhesion molecule (EpCAM) and cytokeratin (CK).
“Cancer cells undergo epithelial–mesenchymal transition (EMT) when they leave the primary tumor site and go into circulation. Therefore, immunofluorescent staining of CTCs using epithelial markers would only detect the few CTCs that still have those epithelial markers, as CTCs that have already started the EMT will lose those markers and will not be detected,” explained Dr. Bahassi, while stating that several studies have shown there sometimes could be 30 to 300 times more CTCs in circulation than what CellSearch was able to detect.
Another method to isolate CTCs is by antibody targeting of white blood cells for removal, followed by collection of untagged CTCs. This is a negative CTC selection technique because CD45 markers are used to remove white blood cells from the sample, leaving CTCs behind. However, Dr. Bahassi reported that the selection of CTCs using this method is often not very efficient and the CTC population is usually highly contaminated with leukocytes. In addition, some CTCs express the CD45 marker, and such CTCs would be eliminated with this method.
The third method to isolate CTCs is sized-based filtration which is based on the fact that CTCs are usually bigger than leukocytes. But the heterogeneity of CTCs is a major obstacle for CTC detection, as some CTCs may be smaller than leukocytes and those small CTCs will not be isolated with this method.
The Use of CTCs for Cancer Management and Predicting Outcomes
The CTC count in whole blood is an independent predictor of progression-free survival (PFS) and overall survival (OS) in several metastatic cancers. The literature has shown that the following CTC counts suggest shorter PFS time:
- Metastatic breast cancer: >5 CTCs/7.5 mL of blood
- Metastatic colorectal cancer: >3 CTCs/7.5 mL of blood
- Metastatic prostate cancer: >5 CTCs/7.5 mL of blood.
Regulatory Approvals for CTC-Based Assays in Oncology
In 2004, the FDA approved the first liquid biopsy test, the CellSearch® CTC enumeration platform, to monitor patients with advanced metastatic breast, colon and prostate cancers based on the cancers’ level of CTCs.
In 2022, the FDA approved Parsortix® PC1 Clinical System, the first FDA-cleared medical device for the capture and harvest of CTCs from metastatic breast cancer (MBC) patient blood for subsequent analysis.
“The Parsortix® PC1 Clinical System is not for enumeration of CDCs, but it is for the capture and harvest of CDCs for potential downstream use in NGS [next-generation sequencing] or other applications,” explained Dr. Bahassi.
Current Challenges and Limitations of CTC-Based Liquid Biopsies
The current challenges and limitations for the use of CTCs as a biomarker in liquid biopsy were highlighted by Dr. Bahassi and include:
- CTCs are present in very low abundance: 1 to 10 CTC/mL of blood
- Blood collection and stability is an issue for CTC detection
- CTCs undergo EMT when they leave the primary tumor site and enter circulation, making their detection using epithelial markers difficult
- CTCs are detected mostly when the patient is in the metastatic stage
- High background of normal cells hampers CTC isolation and detection
- Low sensitivity and high blood volumes are required for CTC detection
- The benefit of using CTCs in treatment decision-making is still unclear.
In addition, Dr. Bahassi stressed that the simple enumeration of CTCs will not contribute significantly to the development of improved or more personalized cancer treatments.
“Adoption of CTC use or other non-ctDNA based plasma biomarkers in routine clinical practice will require robust demonstration of analytical validity, clinical validity and most importantly, clinical utility,” said Dr. Bahassi.
ctDNA-Based Liquid Biopsy in Oncology

cfDNA is all non-encapsulated nucleic acids that shed into circulation during cellular necrosis or apoptosis. Usually, a very small fraction of cfDNA in cancer patients comes from CTCs and tumors, but this can depend on the patient’s tumor type and burden.
The cfDNA that originates from tumors is called circulating tumor DNA (ctDNA). ctDNA can be measured in a patient’s sample to screen for cancer.
Concentration of cfDNA and ctDNA in Cancer Patients
The concentration of cfDNA in healthy subjects is between 0 to 100 ng/mL of blood with an average of 30 ng/mL of blood. In contrast, the cfDNA concentration in the blood of cancer patients varies between 0 to 1,000 ng/mL of blood with an average of 100 ng/mL of blood.
Regarding the concentration of ctDNA, there are 100 to 1,000 copies of ctDNA per 5 mL of blood in patients with advanced tumors, and only around 10 copies of ctDNA in early-stage cancers.
ctDNA in Advanced Malignancies and Concentration of Mutant Fragments
During the webinar, Dr. Bahassi discussed the detection of ctDNA in various late-stage human cancers using data from a study by Bettegowda et al., 2014.
According to this study, detectable levels of ctDNA were found in most patients with metastatic cancers of the bladder, colon, stomach, esophagus, pancreas, breast, or head and neck, as well as patients with melanoma or neuroblastoma and patients with stage III ovarian or liver cancers.
In contrast, the study showed that detectable ctDNA levels were found in less than 50 percent of patients with medulloblastomas or metastatic cancers of the prostate, kidney or thyroid, and less than 10 percent of patients with gliomas. Therefore, the percentage of patients with detectable ctDNA levels varies with tumor type.
The study by Bettegowda et al. also found that concentration of ctDNA varies among patients, even among those patients with the same tumor type.
For instance, in some late-stage cancers like neuroblastoma, the concentration of ctDNA can be very high and in the range of 100,000 to almost 1,000,000 mutant fragments per 5 mL of blood. On the other hand, less than 10 mutant fragments per 5 mL of blood is usually detected in gliomas. The researchers concluded that the concentration of mutant fragments is correlated to the stage of the cancer and the type of cancer.
cfDNA Isolation Techniques
The main process for isolating cfDNA involves centrifugation to remove cells, followed by plasma extraction of cfDNA.
There are several kits that can be used to isolate cfDNA and instruments to measure cfDNA concentrations such as Agilent’s TapeStation, and others. There are also new techniques for NGS library preparations and platforms for cfDNA sequencing.
“As a result of all these techniques, cfDNA is the most advanced liquid biopsy biomarker in the clinic, with several FDA-approved assays and many more being considered for approval,” stated Dr. Bahassi.
The Utility of cfDNA for Cancer Management and Predicting Outcomes
The use of cfDNA for detecting mutant fragments in circulation has been approved for many indications, either for screening, disease monitoring or prognosis.
Dr. Bahassi explained that technological advances in genetic sequencing of cfDNA have enabled liquid biopsies and led to marked increase in the detection of therapeutically-targetable mutations.
An example of the utility of cfDNA in cancer management is for detection of activating epidermal growth factor receptor (EGFR) mutations and T790M mutation in patients with advanced non-small cell lung cancer (NSCLC).
Dr. Bahassi explained that the presence of activating EGFR mutations is usually a good indicator that the patient would respond well to EGFR inhibitors. However, the detection of T790M mutation in patients that are undergoing treatment with EGFR therapy is always indicative of resistance to EGFR inhibitors.
Another instance of the use of cfDNA in cancer management is for the detection of BRCA1/2 mutations and/or ATM alterations in prostate cancer as a companion diagnostic for Olaparib.
Regulatory Approvals for cfDNA-Based Assays in Oncology
“Out of all three liquid biopsy biomarkers — CTCs, cfDNA and exosomes — the most regulatory approvals so far involve cfDNA-based assays, especially in the companion diagnostics space,” said Dr. Bahassi.
According to Dr. Bahassi, there were 22 cfDNA-based assays that were approved by the FDA as of September 7, 2022.
A table with some examples of cfDNA-based assays that are approved by the FDA was presented by Dr. Bahassi during the webinar and is shown in Table 1.
Table 1: Some examples of cfDNA-based assays that are approved by the US FDA.
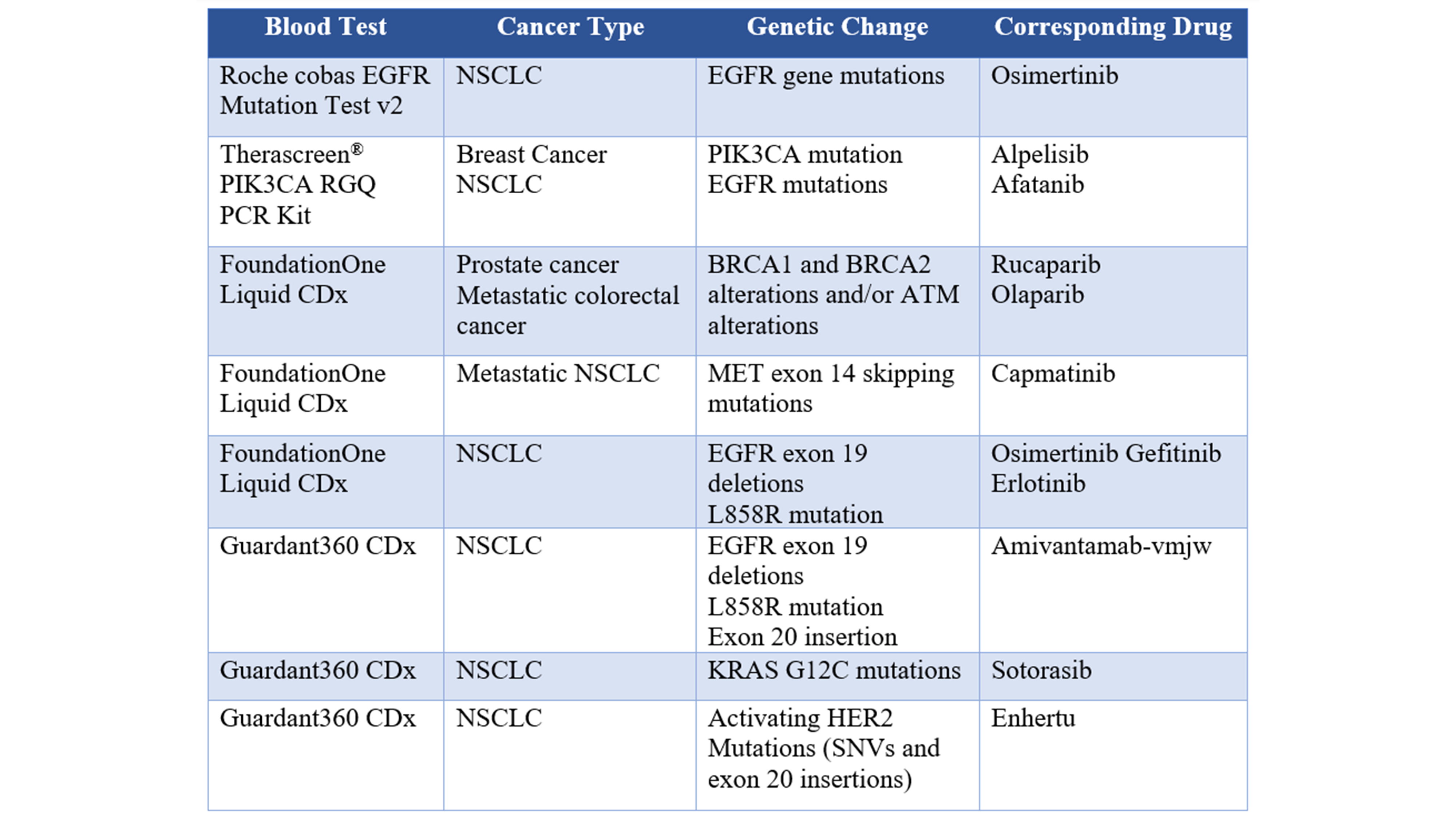
“The leaders in this space now are Foundation Medicine and Guardant360, which have a large number of FDA-approved companion diagnostic assays for different indications,” said Dr. Bahassi.
Detection of Genomic Alterations from cfDNA: Targeted, Non-Personalized Approaches
Non-personalized approaches can be both in-house or through a service provider. The examples presented by Dr. Bahassi include:
- AVENIO ctDNA panels (Roche; in-house solution)
- Oncomine™ Pan-Cancer Cell-Free Assay (ThermoFisher; in-house solution)
- TruSight Oncology 500 ctDNA (Illumina; in-house solution)
- FoundationOne® Liquid CDx (Foundation Medicine; end-to-end commercial provider)
- Guardant360™ (Guardant Health; end-to-end commercial provider).
Detection of Genomic Alterations from cfDNA: Personalized, Targeted Assays
During the webinar, Dr. Bahassi gave a brief schematic of how personalized, targeted assays can be developed to detect somatic mutations from cfDNA (Figure 1).
For personalized, targeted assays, a biopsy of a patient’s tumor or a baseline plasma sample is used as a sample for whole exome sequencing (WES) or whole genome sequencing (WGS) to obtain a list of somatic mutations.
The next step is to design patient-specific multiplex assays to track the patient’s own mutations from ctDNA.
The first option is to design a personalized small NGS gene panel based on the somatic mutations that were detected in the patient, and this can be used for monitoring disease progression. The Signatera™ assay by Natera uses this strategy.
The second option is to detect and quantify a set of somatic mutations by digital PCR.
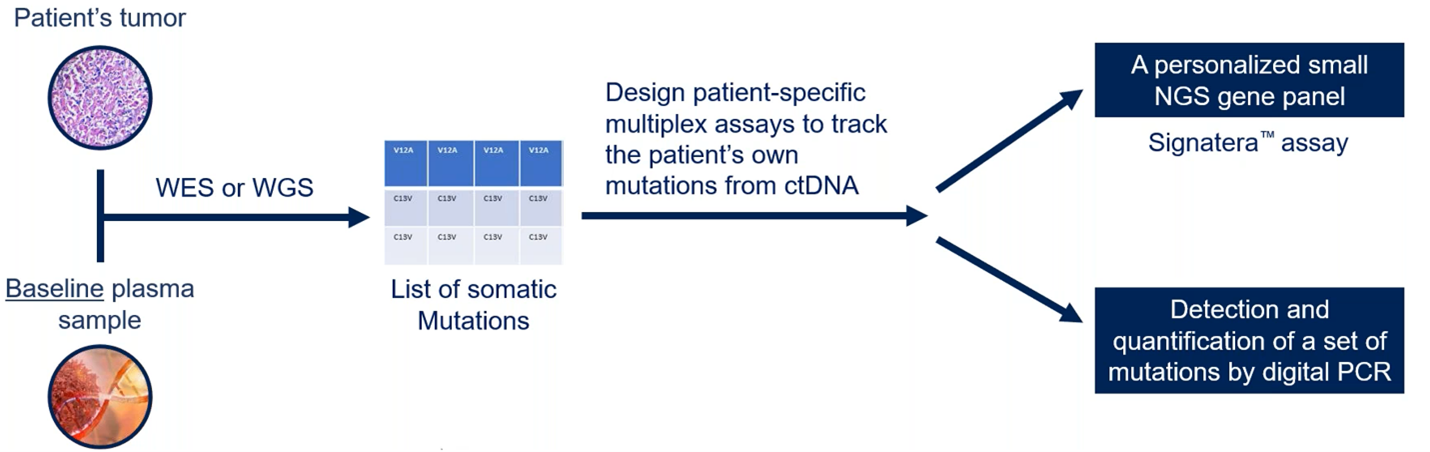
Figure 1. How personalized, targeted assays can be developed to detect somatic mutations from cfDNA.
“A limitation of a personalized, targeted assay is that the mutations detected in a primary tumor may not be the same mutations detected two to three weeks later in plasma during a follow-up of disease progression,” explained Dr. Bahassi. “That is why, for instance with digital PCR, you need to detect and quantify five to ten mutations because some of these mutations may not be there in the near future.”
Current Challenges and Limitations of Liquid Biopsies Based on ctDNA
The current challenges and limitations for the use of ctDNA as a biomarker in liquid biopsy were outlined by Dr. Bahassi and include:
- ctDNA is in very low abundance, especially in early-stage cancers
- Blood collection and stability is an issue for ctDNA detection
- There are no standards to address pre-analytical, analytical and post-analytical criteria
- There is a high risk of false positives and false negatives (variant allele frequencies [VAFs] at frequencies <0.5 percent show less reliability)
- Optimal methods for bioinformatic analysis are still needed.
“Prospective clinical trials are needed to explore whether changing therapy based on ctDNA dynamics prior to radiologic or clinical progression will improve outcomes compared to our current standard,” added Dr. Bahassi.
Exosome-Based Liquid Biopsy in Oncology
Exosomes are extracellular vesicles that contain molecular cargoes (such as various proteins, RNAs and DNAs) specific to the origin cell. Exosomes play a role in cell-to-cell communication and the transmission of diseases.
Exosomes are particularly useful for liquid biopsy tests as they are secreted by living cells rather than secreted during cell death. Therefore, exosome-based assays can offer a more comprehensive, real-time look into a patient’s health. Exosomes are highly stable and easy to obtain and distinguish.
Concentration of Exosomes in Cancer Patients
There are 108 to 109 exosomes/mL in serum or plasma, but a very tiny fraction of these exosomes originate from the tumor. According to Dr. Bahassi, the method of separation can make a big difference in the number of exosomes that are recovered.
Exosome Isolation Techniques
“As there is a high concentration of exosomes in serum or plasma, it makes them relatively easy to obtain,” said Dr. Bahassi.
Another advantage is that exosomes are secreted by living cells and exosomes inherit abundant biological information from their parental cells. Also, exosomes are mostly being used for the detection of circulating RNA and microRNA.
“An additional benefit is that exosomes are innately stable because of their lipid bilayer, and this high biological stability allows for long-term storage of specimens for exosome isolation and detection,” reported Dr. Bahassi.
Multiple platforms have been developed to isolate exosomes using ultracentrifugation (which isolates extracellular vesicles based on size and density), immunoaffinity and filtration.
The Utility of Exosomes for Cancer Management and Predicting Outcomes
Exosomes have shown usefulness in cancer screening, for instance for the detection of ALK fusions in exosomal RNA in lung cancer, and in the detection of BRAFV600E mutation in the lymphatic drainage-derived exosomes in melanoma.
Regulatory Approvals for Exosome-Based Liquid Biopsies
In 2016, ExoDx™ Lung (ALK) was approved for the isolation and analysis of exosomal RNA from blood samples and detection of EML4-ALK mutations in NSCLC.
In 2019, ExoDx Prostate IntelliScore (EPI) was approved by the FDA. EPI provides a risk score to predict whether a patient with PSA from 2 to 10 ng/mL is likely to develop higher-grade prostate cancer based on the detection of ERG, PCA3 and SPDEF RNA in exosomes.
Current Challenges and Limitations of Exosome-Based Liquid Biopsies
During the webinar, Dr. Bahassi outlined these current challenges and limitations for the use of exosomes as a biomarker in liquid biopsy:
- Exosomes are present at low abundance, have high heterogeneity and are nano-sized
- There is limited sensitivity and specificity, low purity and throughput for exosome detection
- No standardized method for exosome detection.
According to Dr. Bahassi, active research is needed to develop an easy-to-operate, high-sensitivity and high-purity platform for exosome separation and detection.
Frequently Asked Questions About Liquid Biopsies in Oncology
Medpace’s recent webinar had a Q&A session where Dr. Bahassi, Dr. Gleich and Dr. Huth answered questions attendees had about the use of liquid biopsy in oncology. Below are the thought-provoking questions from the webinar along with the answers from the experts at Medpace.
What are some regulatory and protocol considerations when enrolling patients into a clinical trial that uses ctDNA as a primary or secondary endpoint?
Dr. Huth: A lot of protocols will have some requirements surrounding lab certification. You might see language around CAP [College of American Pathologists], CLIA [Clinical Laboratory Improvement Amendments], ISO [International Organization for Standardization], IEC [International Electrotechnical Commission] certification required. It’s important that there is certification associated with the results that are obtained. Regulators may ask at some point to provide that documentation, so it’s important to track that across the study.
If a study is enrolling patients in Europe, an important consideration is to make sure that results are coming from CE marked labs due to the implementation of the European Union In Vitro Diagnostics Regulations (EU IVDR).
In addition, even though some studies are allowing liquid biopsy results for enrollment — especially lung cancer and breast cancer studies — protocols may still require the submission of a tissue biopsy.
Dr. Gleich: One of the safety concerns we see, especially from the FDA, is with percutaneous lung tissue biopsy because this procedure carries a risk of pneumothorax. For this reason, there has been a lot of urge to use liquid biopsies from patients with lung cancer.
One of the earlier liquid biopsy tests that got FDA approved was for the T790M mutation in lung cancer, to try to avoid the collection of tissue biopsies for safety reasons. So, there is some compromise in mutation detection, but some potential improvement in reducing risk.
Also, much of the targeted medicine activity that is happening right now is in lung cancer and it is making liquid biopsies particularly important.
Dr. Bahassi: There are several factors to consider when designing a trial that involves ctDNA detection. The timing of ctDNA measurement must be taken into consideration. For instance, a surgery can increase total cfDNA which can hamper ctDNA detection, thus ctDNA measurement could be done four to six weeks post-surgery.
Another example is with patients who are undergoing active treatment with chemotherapy, as that can increase the total cfDNA and affect the sensitivity of ctDNA detection.
Infections and patient weight can also increase total cfDNA and affect the sensitivity of ctDNA detection.
Pregnancy increases total cfDNA and can affect the sensitivity of ctDNA detection, and pregnancy may also influence the initial enrollment in the trial because of toxicities from the treatment.
Will tissue biopsy become obsolete in the future, or will liquid biopsy complement tissue biopsy?
Dr. Gleich: Tissue biopsy is still more or less the gold standard when it is possible to obtain, but tissue biopsy is still far from perfect. There is tumor heterogeneity even within tumors. In addition, the primary tumor and the metastatic tumor might have different profiles, and a tissue biopsy cannot be obtained everywhere.
Taking all this into consideration, tissue biopsy is still the ideal procedure, but liquid biopsy can avoid adverse events for the patient as all tissue biopsies are reasonably invasive unless a sample from cutaneous metastasis is taken. Also, tissue biopsies have varying degrees of toxic risk for the patient depending on which tissue is sampled.
Patients may avoid an invasive tissue biopsy procedure if a liquid biopsy test can determine whether a specific mutation is present that could allow a patient to receive a targeted agent or another specific therapy.
However, certain tumor types do not release CTCs at a level that is good for detection, so a tissue biopsy might still be needed. In addition, liquid biopsy tests may have more utility when there is metastatic disease compared to localized tumors.
In addition to diagnosing cancer, guiding treatment decisions and monitoring treatment resistance, what other applications might be on the horizon for liquid biopsy? May liquid biopsy become the primary source for testing for minimal residual disease (MRD)?
Dr. Gleich: The applications of liquid biopsy are coming along, and the quantity of CTCs are pretty much ready for clinical use in some tumor types.
For lung cancer, years ago we used to divide it by lung adenocarcinoma and lung squamous cell carcinoma, and now almost all recent articles show a chart of which actionable mutations are present in lung cancer. So, whether that initial biopsy is a tissue biopsy or a liquid biopsy, if those mutations can be found and the patient can receive a targeted agent, that might have a great benefit for the patient. This approach is mostly used in lung cancer because of the large number of actionable mutations seen in lung cancer, but the approach is also spreading out to all the other tumor types.
Liquid biopsies are not standardized yet for MRD monitoring, but possibly will be in the future.
Are there any promising liquid biopsy assays for early detection of cancer in asymptomatic patients?
Dr. Bahassi: There are two blood-based early cancer detection tests that are under clinical trial investigation and the results of these tests were presented during the last 2021 ASCO Annual Meeting. These tests showed some intriguing findings in detecting early cancer in asymptomatic patients.
These two tests may be making their way onto the market soon, potentially changing the paradigm in cancer screening.
The first promising blood-based early cancer detection test is in the Galleri study which was developed by Grail, and the company has since been purchased by Illumina. They have found that the test accurately detected cancer signals across more than 50 cancer types with an overall sensitivity of 51 percent.
The second promising blood-based early cancer detection test is the Lunar-2 assay from Guardant Health. Their assay simultaneously interrogates somatic, methylation and fragmentomic signals from ctDNA in the blood.
Those are the two blood-based early cancer detection tests, and the companies are actively pursuing FDA approval.
To learn more about the current liquid biopsy methodologies and how they may help with cancer treatment selection and treatment monitoring, register to watch the free on-demand webinar by Medpace.
This article was created in collaboration with the sponsoring company and the Xtalks editorial team.





Join or login to leave a comment
JOIN LOGIN